Health
Oral sex is now the leading risk factor for throat cancer

HPV is sexually transmitted. For oropharyngeal cancer, the main risk factor is the number of lifetime sexual partners, especially oral sex. (Pexels photo)
Over the past two decades, there has been a rapid increase in throat cancer in the west, to the extent that some have called it an epidemic. This has been due to a large rise in a specific type of throat cancer called oropharyngeal cancer (the area of the tonsils and back of the throat). The main cause of this cancer is the human papillomavirus (HPV), which are also the main cause of cancer of the cervix. Oropharyngeal cancer has now become more common than cervical cancer in the US and the UK.
HPV is sexually transmitted. For oropharyngeal cancer, the main risk factor is the number of lifetime sexual partners, especially oral sex. Those with six or more lifetime oral-sex partners are 8.5 times more likely to develop oropharyngeal cancer than those who do not practise oral sex.
Behavioural trends studies show that oral sex is very prevalent in some countries. In a study that my colleagues and I conducted in almost 1,000 people having tonsillectomy for non-cancer reasons in the UK, 80% of adults reported practising oral sex at some point in their lives. Yet, mercifully, only a small number of those people develop oropharyngeal cancer. Why that is, is not clear.
The prevailing theory is that most of us catch HPV infections and are able to clear them completely. However, a small number of people are not able to get rid of the infection, maybe due to a defect in a particular aspect of their immune system. In those patients, the virus is able to replicate continuously, and over time integrates at random positions into the host’s DNA, some of which can cause the host cells to become cancerous.
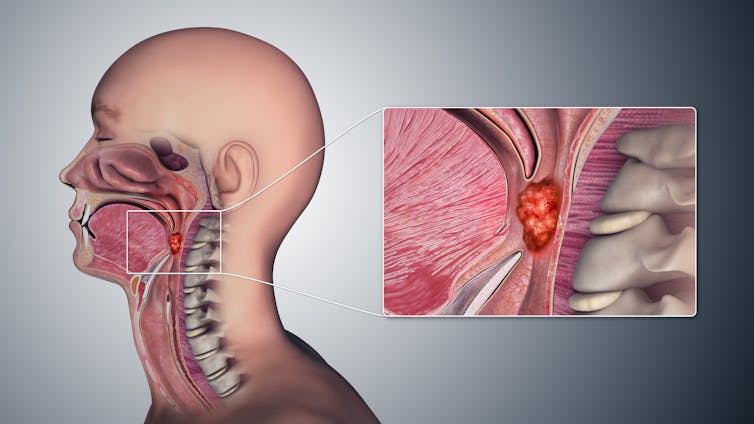
The oropharynx is middle section of the throat (pharynx). Scientific Animations/Wikimedia Commons, CC BY-SA
HPV vaccination of young girls has been implemented in many countries to prevent cervical cancer. There is now increasing, albeit as yet indirect evidence, that it may also be effective in preventing HPV infection in the mouth. There is also some evidence to suggest that boys are also protected by “herd immunity” in countries where there is high vaccine coverage in girls (over 85%). Taken together, this may hopefully lead in a few decades to the reduction of oropharyngeal cancer.
That is well and good from a public health point of view, but only if coverage among girls is high – over 85%, and only if one remains within the covered “herd”. It does not, however, guarantee protection at an individual level – and especially in this age of international travel – if, for example, someone has sex with someone from a country with low coverage. It certainly does not afford protection in countries where vaccine coverage of girls is low, for example, the US where only 54.3% of adolescents aged 13 to 15 years had received two or three HPV vaccination doses in 2020.
Boys should have the HPV vaccine too
This has led several countries, including the UK, Australia and the US, to extend their national recommendations for HPV vaccination to include young boys – called a gender-neutral vaccination policy.
But having a universal vaccination policy does not guarantee coverage. There is a significant proportion of some populations who are opposed to HPV vaccination due to concerns about safety, necessity, or, less commonly, due to concerns about encouraging promiscuity.
Paradoxically, there is some evidence from population studies that, possibly in an effort to abstain from penetrative intercourse, young adults may practise oral sex instead, at least initially.
The coronavirus pandemic has brought its own challenges, too. First, reaching young people at schools was not possible for a period of time. Second, there has been an increasing trend in general vaccine hesitancy, or “anti-vax” attitudes, in many countries, which may also contribute to a reduction in vaccine uptake.
As always when dealing with populations and behaviour, nothing is simple or straightforward.![]()
Hisham Mehanna, Professor, Institute of Cancer and Genomic Sciences, University of Birmingham
This article is republished from The Conversation under a Creative Commons license. Read the original article.



















